PeriOptima: Building an AI Platform for Safer Surgical Care
Co-founded and leading product at a perioperative care platform—from clinical architecture to working prototype—targeting the $75B surgical complications market.
- Shipped fully functional cross-platform prototype: clinical dashboard, patient app (iOS, Android, Web), FHIR backend, and risk engine
- Designed agentic Bayesian risk network integrating 8+ peer-reviewed clinical models from live EHR data
- Architected HIPAA-compliant, FHIR R4 platform with read-only Epic integration requiring zero workflow changes
- Recruited and led founding engineering team; established technical standards and agile workflows from scratch
- Targeting $1–2B beachhead in major surgical complications; $75B category opportunity

The Problem
30 million inpatient operations happen in the US each year. 15% of those patients suffer major postoperative complications. The annual cost: $75 billion.
The system isn’t missing data. It’s missing a platform that connects it.
Risk calculators exist inside EMRs but get calculated manually, if at all. Patients leave the hospital with a printed instruction sheet and a phone number. Monitoring stops at discharge—exactly when complications start to build. When something goes wrong, it surfaces as an unnecessary ED visit or a readmission that costs $17,000 and didn’t need to happen.
Half of surgical patients never receive timely follow-up within the 7–14 day window that catches most complications. Five interconnected failures—incomplete clinical data, unaddressed risk, unsupported patients, monitoring that stops at discharge, and overwhelmed clinical teams—compound each other at every transition. No single platform addresses all five. That’s what we’re building.
What PeriOptima Does
PeriOptima is a perioperative care platform that covers the full surgical journey: pre-op risk stratification through in-hospital recovery through at-home monitoring. It integrates EHR data, patient-reported outcomes, and real-time device data into a single clinical view—then surfaces the signals that matter to the right person at the right time.
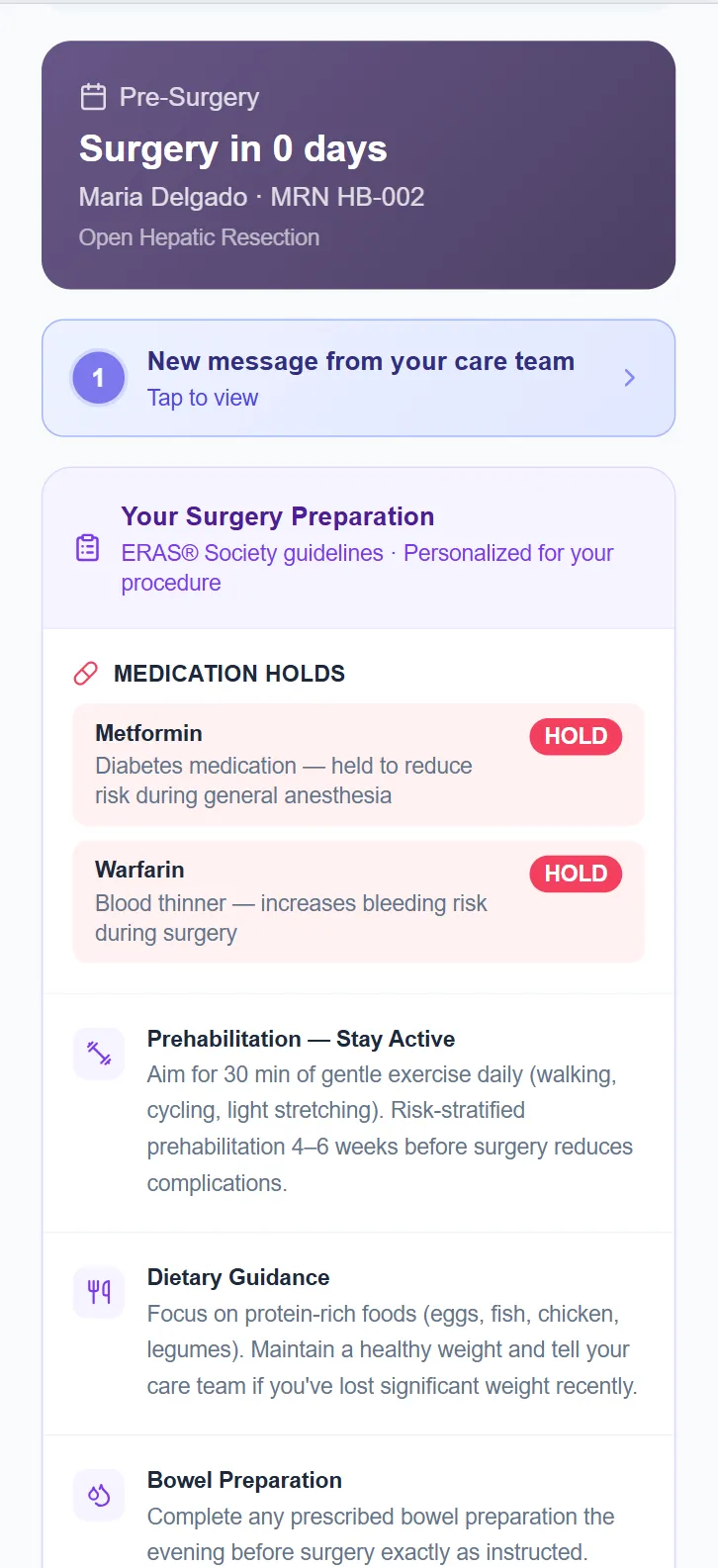
Pre-surgery: Automated risk stratification pulled directly from the patient’s EHR via FHIR, using validated clinical models. A personalized care pathway built from that specific patient’s risk profile—not a generic protocol. Preparation guidance delivered in plain language to the patient’s phone before the first pre-op appointment.
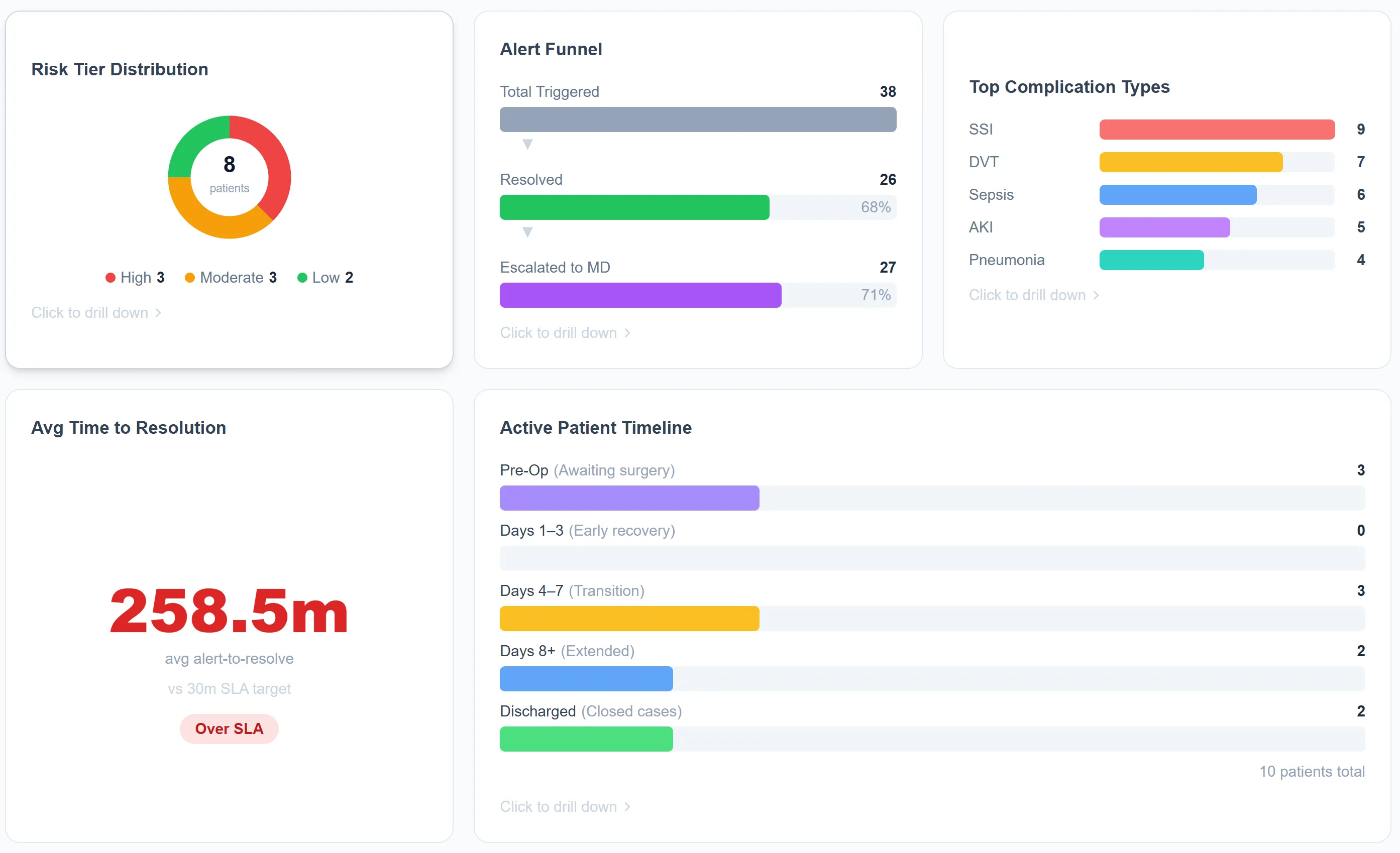
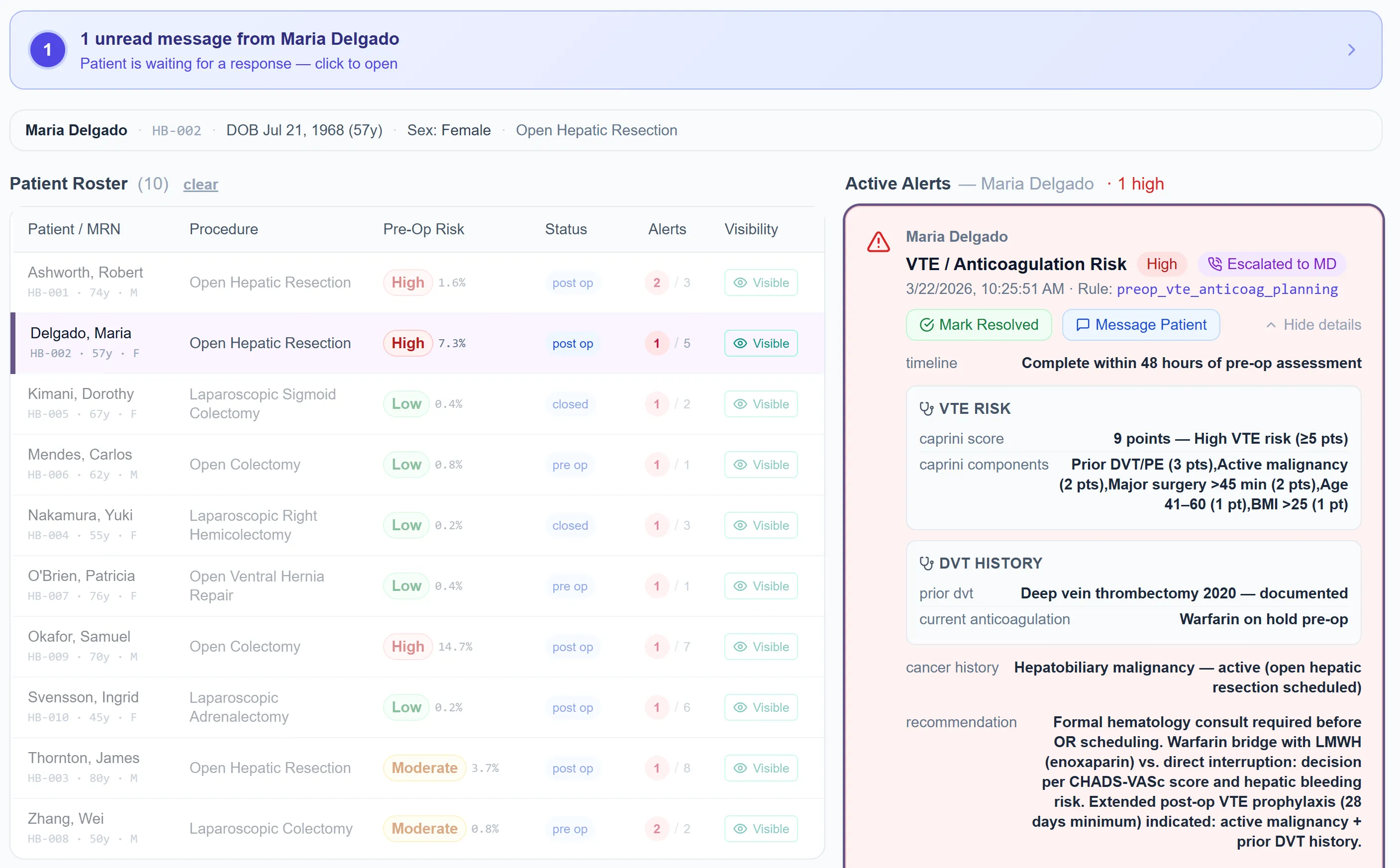
In-hospital: A real-time clinical dashboard with smart alert routing, SLA tracking, and procedure-specific logic. Patients stay engaged through daily symptom check-ins and milestone tracking. The clinical team gets a live cohort view without managing a wall of noise.
At-home recovery: Daily symptom check-ins, continuous vitals via Tenovi RPM devices and HealthKit, wound photo uploads, and secure messaging with the care team. Smart escalation routes urgent concerns to clinicians; routine follow-up runs automatically.
The Risk Engine
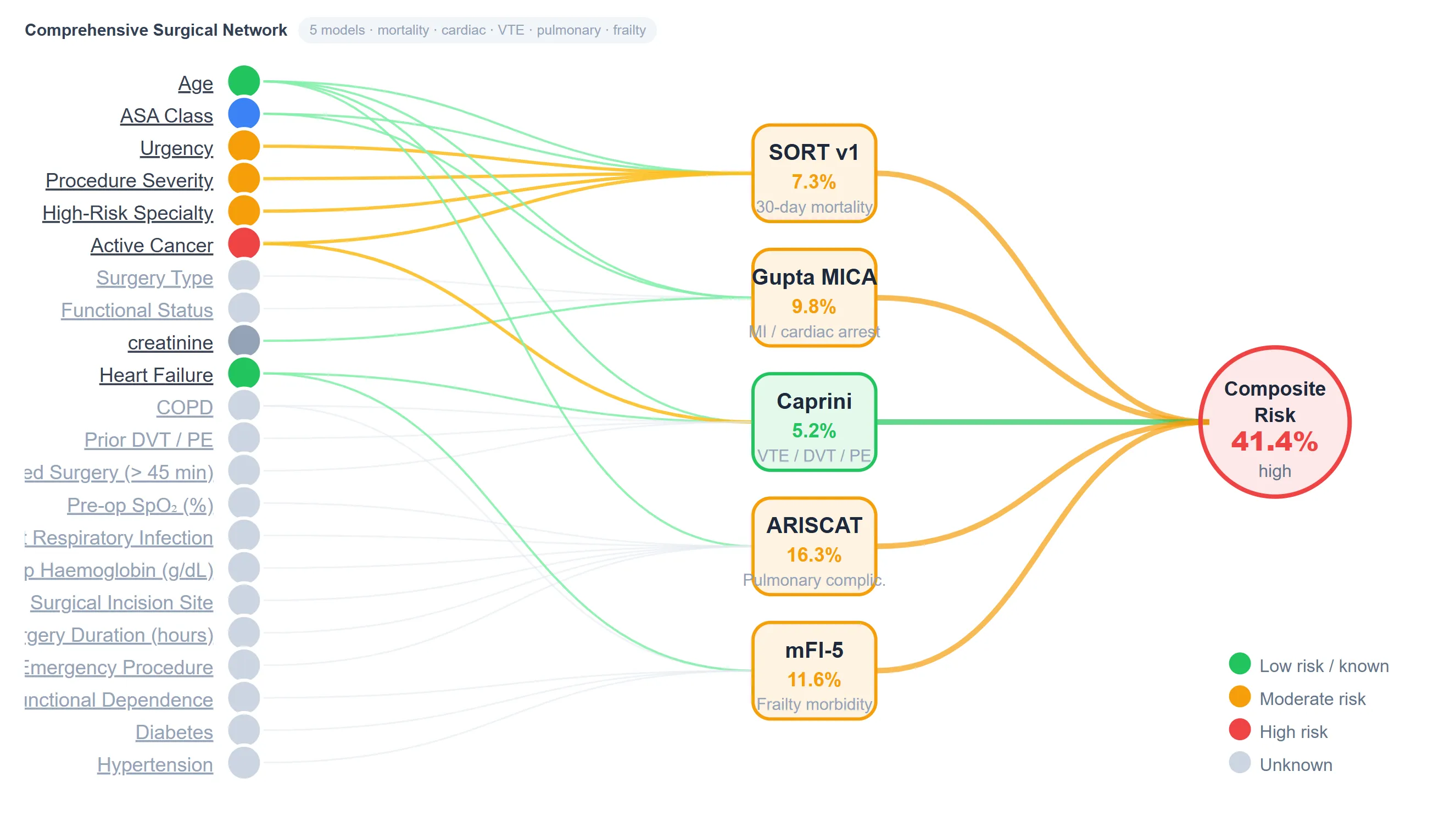
The technical core of PeriOptima is the risk stratification system. I worked directly with our founding AI architect on a Bayesian risk network that doesn’t just calculate individual scores—it models the relationships between clinical inputs and composite risk across multiple validated instruments simultaneously.
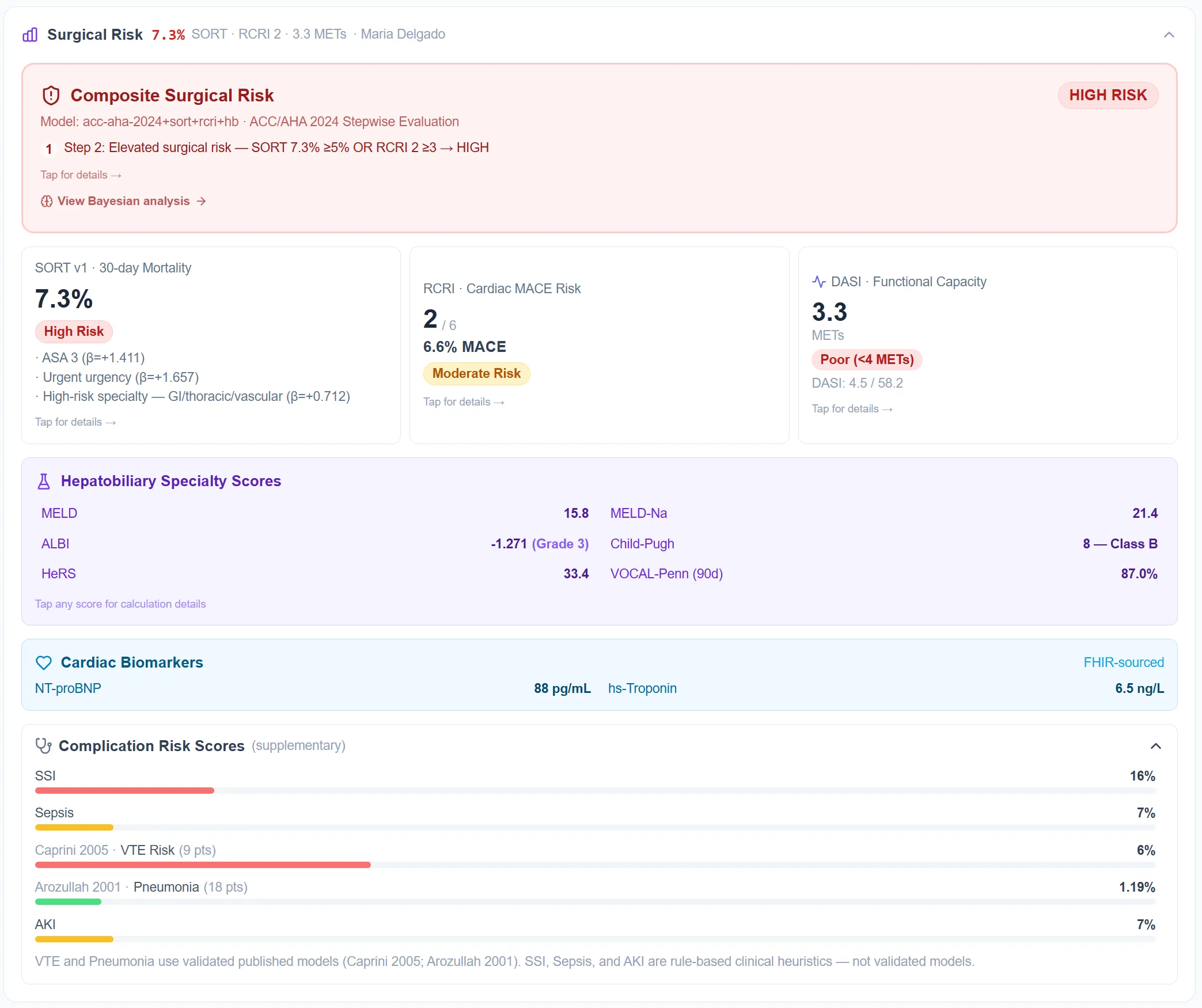
SORT v1 (validated across 4 million procedures) for 30-day surgical mortality. RCRI and DASI for cardiac risk and functional capacity, per ACC-AHA 2024 guidelines. Caprini 2005 for VTE. The full hepatobiliary panel—MELD, ALBI, Child-Pugh, VOCAL-Penn—for hepatic surgery patients. ARISCAT for pulmonary complications. mFI-5 for frailty.
None of this is entered manually. The scores are calculated from the patient’s actual EHR record via FHIR and surfaced before the first appointment. Clinicians can trace exactly which inputs are driving each model—down to the individual variable and its contribution to the composite risk score.
This matters for regulatory reasons as much as clinical ones. Every model is a published, peer-reviewed instrument. Nothing is a black box. The system is built to be explainable to the patient, the surgical team, and, eventually, the FDA.
The Patient App
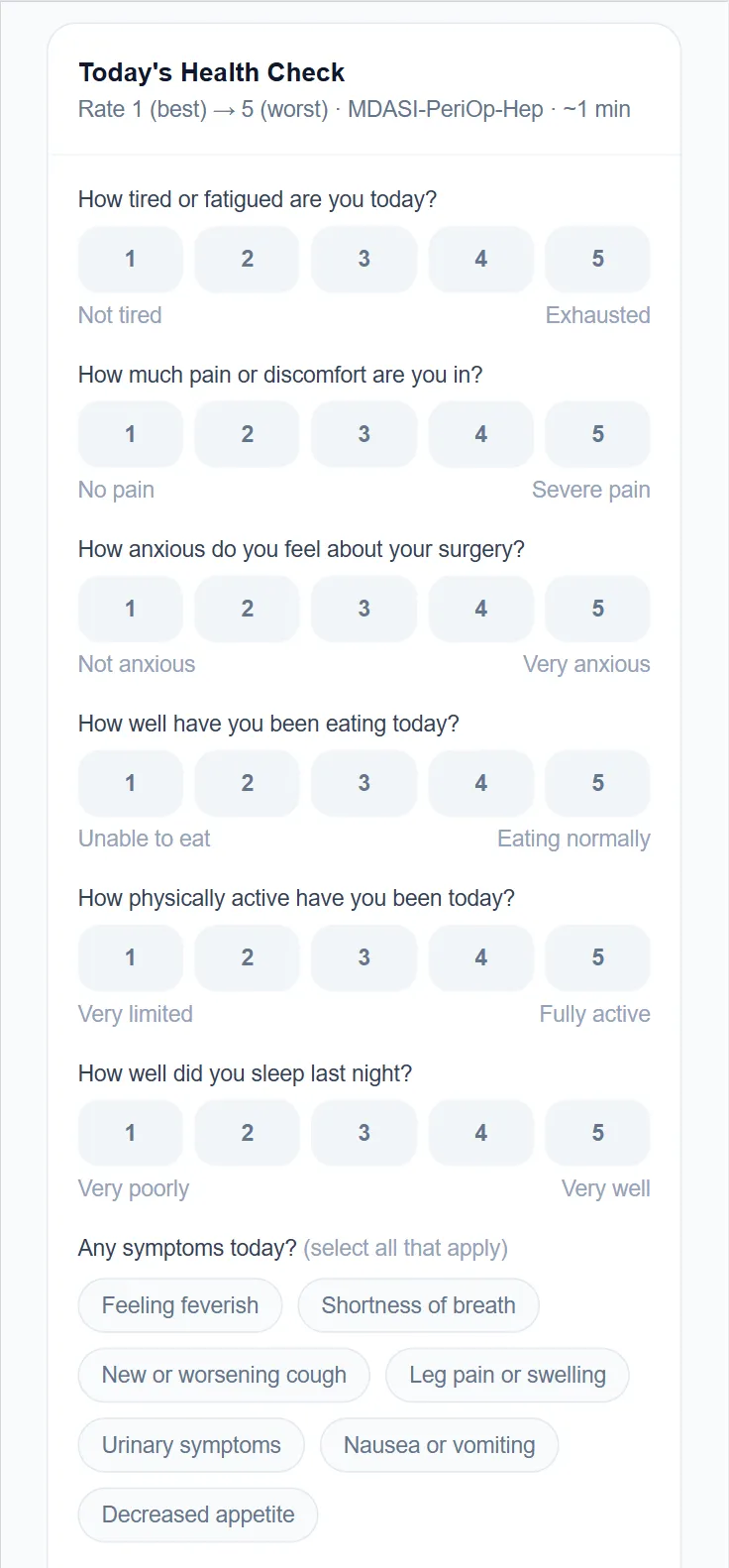
Patients experience PeriOptima through a cross-platform mobile app on iOS, Android, and Web. The clinical sophistication is invisible to them. What they see is a preparation guide that actually fits their situation, a daily check-in that takes about a minute, recovery guidance in plain language, and a direct line to their care team.
Before surgery, the app surfaces medication holds, prehabilitation targets, dietary guidance, and bowel preparation steps—all derived from their specific risk profile and procedure type. Functional capacity is assessed through a DASI questionnaire presented as a simple activity survey. Their answers feed directly into the cardiac risk calculation.
At home, the app becomes a recovery guide: ERAS Society guidelines personalized to their procedure, daily vitals via connected devices, wound photo uploads, and a 24/7 AI recovery assistant for questions about wound care, diet, and activity. When a patient messaged her care team at 3:30am to ask whether coffee counted as a meal before her Ursodiol dose, her team answered before morning rounds—instead of an unnecessary ED visit.
Monitoring and Response
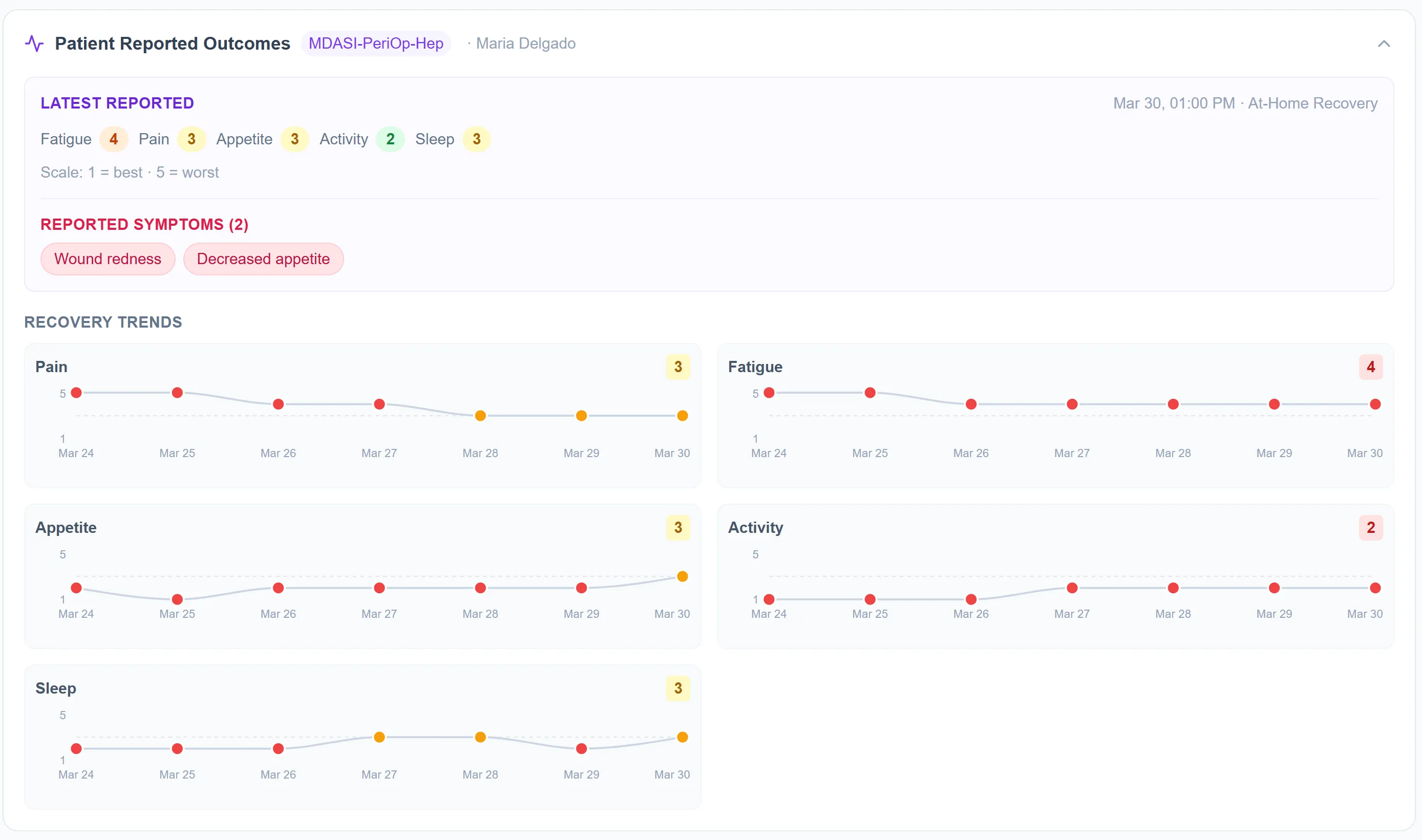
The connection between patient and clinical team doesn’t break at discharge. Vitals stream continuously from Tenovi Pulse Ox and blood pressure monitors into the clinical record. Patient-reported outcomes—pain, fatigue, appetite, activity, sleep—via the MDASI-PeriOp instrument generate longitudinal trends the care team can see building over days.
When a patient’s pain score is rising over five consecutive days, or SpO₂ is declining, the system flags it before it becomes acute. The care team isn’t monitoring constantly—they’re notified when a patient needs them. Everything else is handled automatically.

Building It
I co-founded PeriOptima with Adam Schlifke, a board-certified anesthesiologist from Stanford and Kaiser, after working directly with surgeons and anesthesiologists to understand where the clinical system actually breaks down. The product strategy came from translating those clinical conversations into a platform architecture.
I set the product vision, defined the three-phase care journey framework, and led every major product initiative from the start. I built the first working prototype before the engineering team was fully in place—cross-platform app, FHIR backend, risk engine—the same way I built ADHDAlly as a solo founder. Once we began hiring, I recruited the founding engineers, established agile workflows and technical standards, and have continued contributing to the codebase alongside the team.
CTO Kul Bhushan joined several months in, bringing regulatory depth, FHIR expertise, and healthcare compliance structure. The integration architecture—read-only Epic via FHIR R4, zero workflow changes for clinical staff—is a product of that collaboration. I brought perspective on data orchestration, agentic evaluation pipelines, and what the “complete clinical picture” actually requires at the data layer. Kul brought the structure to make it compliant and operable inside a health system.
The founding team now includes a CMO (MD/MBA, Kaiser/Deloitte), a COO with deep digital health infrastructure experience, a CFO with SaaS and M&A background, three founding engineers, a Stanford GSB board member, and a clinical advisory bench covering anesthesiology, surgery, liver transplant, and health IT.
Where We Are
PeriOptima is pre-pilot. We have a fully functional prototype, a founding team in place, and active investor conversations underway. We’re scoping a 90-day pilot structure with target health systems: 50–100 patients, read-only Epic integration, zero workflow disruption.
The ROI case for a hospital running 8,600 inpatient procedures annually is specific: a 10% reduction in perioperative costs produces $5.36M in annual savings against a $500K platform cost. 10:1 return.
The beachhead market is $1–2B in major surgery complications. The category opportunity is $75B. The clinical models are validated. The platform works. What we’re building next is the evidence base to prove it at scale.